This has been making the rounds on Facebook lately, so perhaps you've seen this but if not it is definitely worth checking out. In an effort to boost the country's morale and whip them into shape for the upcoming 2014 Sochi Winter Olympics, the Russian Olympic Committee installed ticket vending machines that accepted 30 squats instead of 30 rubles for one ticket. It's a great idea and maybe something Translink in Vancouver should consider before it launches the new Compass system... 30 squats for a ticket, yoga class for an all-day ticket, run a marathon for a month pass? Could be a hit around these parts. If not, maybe we could all start busting out some squats before hopping on the train anyways? Let me know if you're with me.
Check out the video here!
Have a great weekend everyone!
Saturday, 23 November 2013
Friday, 15 November 2013
Something new (sort of...) to learn about the knee!
Hello everyone!
The semester came out swinging on these bloggers and before we knew it, two months had gone by without getting our first post up when we wanted it. Sorry about that, but going forwards into the end of 2013 and the start of 2014 we can keep you updated with what sort of fun stuff we're doing at Naturopathic Med school, tips to study and any other interesting articles in regards to anatomy, medicine and health.
Hopefully everyone heard and got as excited about the anterolateral ligament (ALL) as me when this study was published by researchers in Belgium. However, turns out (as their abstract states) this structure had been observed as early as 1879 by Paul Segond, a surgeon from France. He described a 'pearly, resistant, fibrous band' at the anterolateral aspect of the knee, but it took until 2013 for these researchers to provide a full anatomical description.
They found that in 40/41 (97%) of cadavers dissected, the ALL was 'a well-defined ligamentous structure, clearly distinguishable from the anterolateral joint capsule,' and that it ran from the lateral femoral epicondyle to the anterolateral tibia with firm insertions to the lateral meniscus along the way.

The semester came out swinging on these bloggers and before we knew it, two months had gone by without getting our first post up when we wanted it. Sorry about that, but going forwards into the end of 2013 and the start of 2014 we can keep you updated with what sort of fun stuff we're doing at Naturopathic Med school, tips to study and any other interesting articles in regards to anatomy, medicine and health.
Hopefully everyone heard and got as excited about the anterolateral ligament (ALL) as me when this study was published by researchers in Belgium. However, turns out (as their abstract states) this structure had been observed as early as 1879 by Paul Segond, a surgeon from France. He described a 'pearly, resistant, fibrous band' at the anterolateral aspect of the knee, but it took until 2013 for these researchers to provide a full anatomical description.
They found that in 40/41 (97%) of cadavers dissected, the ALL was 'a well-defined ligamentous structure, clearly distinguishable from the anterolateral joint capsule,' and that it ran from the lateral femoral epicondyle to the anterolateral tibia with firm insertions to the lateral meniscus along the way.

So what's important about this? Researchers believe that the ALL plays an important role in patients ACL tears. The Belgian doctors were finding that even after patients had reconstructive ACL surgery, they still experienced pivot shift episodes where the knee would give out and they would lose stability. Due to the common nature of these tears in athletes playing a wide variety of sports, fully understanding this ligament may allow doctors to treat patients with ACL tears more effectively in the future.
If you're interested in reading more about this 're-discovery', make sure to check out the abstract at the top and take a read through this New York Times article.
For more information on the knee and performing a proper knee exam, check out Pro Health System's website!
Tuesday, 25 June 2013
The Importance of a Good Physical Exam
Another link for people to check out this week as we steadily progress through exams... I can see the light!
This clip may deal with the relationship between Radiology and the Emergency Room, but that is just one situation where a good clinical exam is so important. Having the skills to properly inspect a patient is something every physician requires or you might end up in a frustrating conversation like this... Let's just hope that one of you aren't the one with the IQ of french fries. Enjoy!
http://www.youtube.com/watch?v=Es1TtaVXO2I&feature=youtube_gdata_player
This clip may deal with the relationship between Radiology and the Emergency Room, but that is just one situation where a good clinical exam is so important. Having the skills to properly inspect a patient is something every physician requires or you might end up in a frustrating conversation like this... Let's just hope that one of you aren't the one with the IQ of french fries. Enjoy!
http://www.youtube.com/watch?v=Es1TtaVXO2I&feature=youtube_gdata_player
Tuesday, 18 June 2013
Fibrodysplasia Ossificans Progressiva
Hello there! Finals are upon us at Boucher and as such, everyone is in a bit of a time crunch. This week I'm linking you to an interesting article I read on The Atlantic which consistently has well-written articles on health, wellness and medicine. I found this one to be particularly fascinating as we were covering bone and bone development at the time in our Biomed class.
It's a little bit of a read, but well worth it. Click here to read about FOP and the girl who turned to bone.
It's a little bit of a read, but well worth it. Click here to read about FOP and the girl who turned to bone.
Wednesday, 12 June 2013
Osgood-Schlatter Disease
Having sore knees is both painful and frustrating whether you're a 75 year old out for a walk or a 12 year old sidelined at football practice. I was the latter- for a few summers, I was the husky youngster that over-exerted myself and wound up with Osgood-Schlatter disease. Luckily, mine was a very minor case and after football practice I recovered with adequate rest and ice. Others, however, may take weeks to months for recovery and could possibly deal with this issue well into adulthood.
What is it?
Osgood-Schlatter disease is characterized by:
How to treat it
For most kids, R.I.C.E. (see our previous post to refresh your memory on dealing with inflammation) will do the trick. The period of rest will differ for each young athlete- in my case, I would usually need a few days between practices or games to feel ready to run again, others may take as long as 4 weeks. In mature patients, surgery does become an option if the skeleton is fully grown but the knees are still bothered by Osgood-Schlatters.
For more information on Osgood-Schlatter disease and many others, check out the Professional Health Conditions Manual.
Also, if you're looking to take your studying with you on the go, download the new ProHealth App from the iTunes store FOR FREE until the end of the month! It's an easy to use and informative app that lets you take much of the Professional Health Muscle Manual with you on your iPhone or iPad. All you have to do is search "ProHealth" on iTunes to find it and you will be on your way with an excellent new tool to excel in your studies.
What is it?
Osgood-Schlatter disease is characterized by:
- An enlargement of the tibial tuberosity, just below the patella, that is painful and tender
- Knee pain that worsens with activity- running, jumping, climbing etc- and improves with rest
- Tightness of the surrounding muscles, especially the thigh muscles
 |
| A typical image of someone suffering from Osgood-Schlatter disease Source: http://louisvilleorthopedics.com/ |
How does it happen?
 |
| A nice side angle showing where the patellar ligament pulls away from the tibial tubercle. Source: http://www.laserhealthsolutions.com |
Osgood-Schlatter disease happens by repeated stress on the tibia by the patellar ligament (also known as the patellar tendon), which is pulled by the quadriceps every time they are engaged. As the quads are used and pull on that tendon, it may pull away from the tibial tuberosity (or tubercle), resulting in the pain and swelling that is common with the disease. If the issue is not treated, it may progress far enough to be a full avulsion fracture. Overtime, the adolescent's bone may try to heal itself and close that gap with new bone growth- this is going to result in a bony lump at that spot.
 |
| Contraction of the powerful quadricep muscles will cause irritation of the patellar tendon and tibial tuberosity. Source: http://activerelease.ca/wordpress/ |
How to treat it
For most kids, R.I.C.E. (see our previous post to refresh your memory on dealing with inflammation) will do the trick. The period of rest will differ for each young athlete- in my case, I would usually need a few days between practices or games to feel ready to run again, others may take as long as 4 weeks. In mature patients, surgery does become an option if the skeleton is fully grown but the knees are still bothered by Osgood-Schlatters.
For more information on Osgood-Schlatter disease and many others, check out the Professional Health Conditions Manual.
Also, if you're looking to take your studying with you on the go, download the new ProHealth App from the iTunes store FOR FREE until the end of the month! It's an easy to use and informative app that lets you take much of the Professional Health Muscle Manual with you on your iPhone or iPad. All you have to do is search "ProHealth" on iTunes to find it and you will be on your way with an excellent new tool to excel in your studies.
Tuesday, 11 June 2013
ProHealth App
Good evening everyone! Exciting news from Professional Health Systems. Our new app is up and running on iTunes for you to download, and make sure you do it soon as it is FREE until the end of the month. The app includes flash cards that will help you study or brush up on your anatomy wherever you are. If you're the type of person who suddenly has the urge to know which muscles help you chew or what the anconeus muscle does, then this app is for you.
If you download it and have any feedback at all, we would love to hear it! Get back at us on the blog with any comments you may have.
If you download it and have any feedback at all, we would love to hear it! Get back at us on the blog with any comments you may have.
Friday, 7 June 2013
The Limb Numbing Lumbar Disc Herniation
Can you do this without feeling any numbness below your knee or pain in your hip? If no...well you just MIGHT have a disc herniation.
What exactly is a Disc Herniation?
 |
| Source: http://www.backpainhelptoday.com/herniated-disc/ |
 |
Source: http://www.columbianeurosurgery.org/wp-content/2009/11/sc.gif |
The "disc" in disc herniation is referring to the intervertebral disc (seen on the right, but also in blue below) that can be likened to a jelly doughnut. The "jelly" on the inside is called the nucleus pulposus (in white) and the "doughnut" is a ligamentous structure called the anulus fibrosus (in pink).
Simply put, a disc herniation is a tear in the anulus fibrosus which leads to the protrusion/bulging of the nucleus pulposus. This bulge can compress a nerve root which may cause symptoms seen in a disc herniation.
These bulges can be either posterior or lateral (depending on where the ligament tears), but they occur most commonly at the L4-L5 or L5-S1 spinal level.
What is the cause of disc herniation and what are the symptoms?
Symptoms include:
- Low back pain (at first) because you have sprained your back (torn those ligaments)
- Numbness and tingling into extremity in a dermatonal pattern, usually L5-S1 (refer to page 360 - 361 in the Muscle Manual for a map of the dermatones)
What confirmatory tests can be performed?
Straight Leg Raise Test
When you are at the apex (or at the maximum point where there is no reproduction of symptoms) and have dorsiflexed the foot, bend the knee and continue to flex the hip to rule out any hip problems. A positive test will show possible sciatic nerve impingement due to disc herniation.
Deep Tendon Reflex (DTR)
For disc herniations, the "ankle jerk" reflexes (testing L5-S1) is most applicable. An abnormal reflex (must perform test bilaterally to determine what's considered normal for the patient) may confirm lumbar disc herniation, but other tests must be performed.
Resisted dorisflexion test
The patient will dorsiflex as shown in the video, but instead of the elastic band, the practitioner will push the patient's foot into plantar flexion and the patient will be asked to resist their force. If the patient cannot (or weakly can) resist the practitioner's force, it may confirm a disc herniation impinging the sciatic nerve.
Treatment of a disc herniation
Acute Disc Herniation:
- Decrease inflammation (via PRICE) and decrease load bearing
- Avoid any twisting or aggravating activity (especially the activity that caused the injury in the first place)
- Lock the pelvis in a neutral position for any movements (to protect the back and decrease potential for further injury)
Chronic Disc Herniation:
- Spinal decompression
- There are several ways to decompress the spine:
- Inversion table
- Decompression machine
- Hanging from a stable door/bar
- Simply laying down (takes the pressure off the spine and allows for re-hydration of discs)
A disc herniation should resolve itself IF you deal with it EARLY/ACUTELY, don't wait until it becomes chronic and a major problem! If you want to be able to kick and stretch at 50 like Sally O'Malley, PROTECT THAT BACK and get it looked at early!
Tuesday, 4 June 2013
The Hip!
No, not the Tragically Hip... which would possibly make for a more interesting article, who doesn’t love Gord Downie and the boys? Instead today we’re going to have an overview of the hip and some aspects of it that are important for everyone to understand.
 |
| Great hip flexion Mr. Downie! But not the point of this post. Source: www.windsorstar.com |
Depending on who you ask, the hip can mean different things. It’s a large area and it is vital to differentiate between the hip joint, the hip bone, the sacroiliac joint or soft tissue surrounding the area. Often, patients will present with pain saying that their hip hurts and be pointing vaguely to somewhere near the iliac crest or perhaps their anterior superior iliac spine. While these are part of the hip bone, also known as your pelvic or coxal bone, it’s important to have a good understanding of the hip to help you discern exactly which structure the patient is talking about.
 |
| Source: Gray's Anatomy |
 |
| The left hip bone with a good view of the acetabulum where the femoral head sits. Source: Gray's Anatomy |
The hip bone is actually made up of three bones- the ilium, ischium and pubis, which do not finish fusing together until approximately age 25. The hip bones come together anteriorly at the pubic symphysis and posteriorly at the two sacroiliac joints. An important thing to remember is that three of the SI joint ligaments (sacrotuberous ligament, sacrospinus ligament and sacroiliac ligament) are three of the strongest you will find in the human body. The hip bone has a myriad of important muscular attachments, some of these include the quadratus lumborum, iliacus, gluteus max, med and min. Pictures help for a better understanding of all the bone structure and muscle attachments in this area and The Pro Health Muscle Manual is a great tool to help you learn. On the lateral side of the hip bone is where you will find your hip joint, also known as the acetabulofemoral joint (because of the hip structure acetabulum creating a ball and socket joint with the head of the femur). This is the area replaced when you hear about somebody getting a hip replacement (not for the squeamish). For more information on both the anatomy of this area and testing it, check out the Physical Assessment Manual.
Another area of the hip bone worth mentioning is the ischial tuberosity. I don’t know how many of you practice yoga, but if you have ever heard a teacher tell you to “root down into your sit bones” and not know what the heck they were talking about, this is it. Your ischial tuberosity is the bony segment you can feel if you pull a cheek away while sitting on your bottom, and it really helps you find stability on the floor for seated postures. It’s an important anatomical location in yoga (check out this article for a better understanding) and also in everyday anatomy. The ischial tuberosity wraps around towards the pubis bone, creating a space known as our obturator foramen which allows the passage of blood vessels and nerves.
 |
An excellent picture from Gray's showing all three bones of the hip bone and
the Ischial Tuberosity (Tuberosity of Ischium). Source: Gray's Anatomy
|
Hip injuries are a common issue today. Maybe it’s an athlete with a hip flexor problem, the development of osteoarthritis in the hip joint, or the unfortunate case of an elderly person falling and breaking their hip. All of these problems will require a thorough understanding of the hip’s anatomy and if you want solid resources to learn from or supplement your practice with, take a look at Pro Health’s full line of products.
Friday, 24 May 2013
Inflammation: what causes it, cardinal signs, and natural approaches to deal with inflammation
What causes inflammation?
Inflammation is not as evil as its made out to be. It is completely natural! It is your body's way of protecting itself from anything harmful or irritating such as chemical irritants, any damaged cells, or pathogens. Inflammation is your body telling you that it's trying to heal itself from a harmful stimuli.
Of course, inflammation is only good to a limited extent. Acute inflammation is GREAT for your body to increase blood flow to the area and fight the harmful stimuli. However, chronic inflammation may prove to have negative consequences as the accumulation of chemicals and by-products of the inflammatory response may cause stress to your body, which may, in turn, impede in your immune function.
Cardinal signs of inflammation
The easiest way to remember the cardinal signs of inflammation is:
Inflammation caused by a SHARP needle.
Swelling
Heat
A loss of function
Redness
Pain
The more superficial the inflammation is, the more of the cardinal signs you will see. But remember, just because you don't see all of the signs does not mean that inflammation is not present.
Dealing with inflammation...naturally!
Curcumin (the active constituent found in turmeric) has been the "up-in-comer" for the treatment of inflammation. According to Satoskar, a double blind, placebo-controlled clinical trial on post-operative patients found that curcumin was more effective than phenylbutazone and placebo in the treatment of post-operative inflammation (2004).
Recently, there has been extensive research in the biological activities and pharmacological actions of turmeric and its constituents (i.e. curcumin). Here are two papers that have been published about the anti-inflammatory action of curcmin:
Sources:
1) Satoskar RR, Shah SJ, Shenoy SG. Evaluation of anti-inflammatory property of curcumin (diferuloyl methane) in patients with postoperative inflammation. Int J Clin Pharmacol Ther Toxicol 1986;24(12):651-54. Cited in Mills S, Bone K. Principles and Practice of Phytotherapy: Modern
How do you deal with inflammation?
What are your thoughts about the anti-inflammatory actions of Curcumin discussed in the papers?
Comment below!
Inflammation is not as evil as its made out to be. It is completely natural! It is your body's way of protecting itself from anything harmful or irritating such as chemical irritants, any damaged cells, or pathogens. Inflammation is your body telling you that it's trying to heal itself from a harmful stimuli.
Of course, inflammation is only good to a limited extent. Acute inflammation is GREAT for your body to increase blood flow to the area and fight the harmful stimuli. However, chronic inflammation may prove to have negative consequences as the accumulation of chemicals and by-products of the inflammatory response may cause stress to your body, which may, in turn, impede in your immune function.
Cardinal signs of inflammation
The easiest way to remember the cardinal signs of inflammation is:
Inflammation caused by a SHARP needle.
 |
| Source: http://en.wikipedia.org/wiki/Inflammation |
Heat
A loss of function
Redness
Pain
The more superficial the inflammation is, the more of the cardinal signs you will see. But remember, just because you don't see all of the signs does not mean that inflammation is not present.
Dealing with inflammation...naturally!
- To decrease inflammation after an acute injury make sure you remember PRICE
- If you don't know or remember what PRICE is, check out "The Infamous Ankle Sprain" post to find out!
- Contrast Hydrotherapy
- Simply alternating hot and cold applications to the inflamed area.
- The cold application will decrease chemical reaction speeds thus slowing down the inflammatory response.
- The hot application will increase blood flow to the injured area and help speed the healing process
- Botanicals
- There are SEVERAL constituents that have anti-inflammatory actions, such as tannins, salicylic acid, and flavones.
- Plants that have anti-inflammatory actions include Calendula (Calendula off.), Chamomile (Chamomilla recutita), and Turmeric (Curcuma longa)
Curcumin (the active constituent found in turmeric) has been the "up-in-comer" for the treatment of inflammation. According to Satoskar, a double blind, placebo-controlled clinical trial on post-operative patients found that curcumin was more effective than phenylbutazone and placebo in the treatment of post-operative inflammation (2004).
Recently, there has been extensive research in the biological activities and pharmacological actions of turmeric and its constituents (i.e. curcumin). Here are two papers that have been published about the anti-inflammatory action of curcmin:
- Anti-inflammatory Properties of Curcumin, a Major Constitutent of Curcuma Longa
- Turmeric and Curcumin: Biological actions and medicinal applications
Sources:
1) Satoskar RR, Shah SJ, Shenoy SG. Evaluation of anti-inflammatory property of curcumin (diferuloyl methane) in patients with postoperative inflammation. Int J Clin Pharmacol Ther Toxicol 1986;24(12):651-54. Cited in Mills S, Bone K. Principles and Practice of Phytotherapy: Modern
How do you deal with inflammation?
What are your thoughts about the anti-inflammatory actions of Curcumin discussed in the papers?
Comment below!
Wednesday, 22 May 2013
The Axillary Artery, Its Branches and Tips for Studying It
As we all know, the flow of blood through the body plays a vital role. Without it, our cells would not receive oxygen and nourishment, metabolic waste would not be cleared out and our health would suffer because of it. When a patient is examined, it's necessary to have a good clinical understanding of the venous and arterial pathways. In cases of ischemia and hypoxia, it's important to know what tissues could suffer and what concerns need to be addressed.
Using this table is a start to good studying for remembering this area, but let me recommend a few more that I have found helpful. Visualizing yourself as a red blood cell and imagining your pathway through the body helps: starting in the aorta, moving through the subclavian artery, continuing down the axillary artery and then taking a sharp turn into the subscapular artery to supply the subscapularis as it is hard at work swimming or throwing a baseball.
Secondly, use mnemonics! Med students have come up with all sorts of interesting mnemonics for remembering different sorts of information (the funniest in my mind have been for the cranial nerves). The axillary artery is no different: Screw The Lawyer Save A Patient moves you through sections one to three in descending order and the arteries that branch off.
There are a few more that you can find here but I encourage you to come up with some of your own. Be creative, be funny and maybe a little rude- those seem to stick the best. We'd love to hear some feedback from you with some of your favourites, so if you have any that come to mind jot them down in the comments section.
And if you are looking for more ways to learn about or become more proficient with anatomy, physical assessment, physical medicine or clinical conditions take a look at our products, thanks!
Today, we'll take a closer look at the axillary artery, the pathways it branches off to, the areas served and a few good study ideas to learn, remember and understand this area. The axillary artery is a continuation of the subclavian artery and has three sections before becoming the brachial artery (after it passes the inferior border of teres major). The three sections can be broken down based on what branches off of them.


The Axillary Artery and its branches. The labels are in small font, try to pick them out and label them yourself! Picture from Gray's Anatomy.
Section
|
Branches
|
Areas Supplied
|
One
|
Superior Thoracic Artery
|
Upper part of thoracic cavity
|
Two
|
Thoracoacromial Artery
|
Pectoral and deltoid regions
|
Lateral Thoracic Artery
|
Lateral structures of thorax
|
|
Three
|
Subscapular Artery
|
Subscapular region
|
Anterior Circumflex Humeral Artery
|
Proximal end of humerus
|
|
Posterior Circumflex Humeral Artery
|
Proximal end of humerus
|
Using this table is a start to good studying for remembering this area, but let me recommend a few more that I have found helpful. Visualizing yourself as a red blood cell and imagining your pathway through the body helps: starting in the aorta, moving through the subclavian artery, continuing down the axillary artery and then taking a sharp turn into the subscapular artery to supply the subscapularis as it is hard at work swimming or throwing a baseball.
Secondly, use mnemonics! Med students have come up with all sorts of interesting mnemonics for remembering different sorts of information (the funniest in my mind have been for the cranial nerves). The axillary artery is no different: Screw The Lawyer Save A Patient moves you through sections one to three in descending order and the arteries that branch off.
There are a few more that you can find here but I encourage you to come up with some of your own. Be creative, be funny and maybe a little rude- those seem to stick the best. We'd love to hear some feedback from you with some of your favourites, so if you have any that come to mind jot them down in the comments section.
And if you are looking for more ways to learn about or become more proficient with anatomy, physical assessment, physical medicine or clinical conditions take a look at our products, thanks!
Saturday, 18 May 2013
The Infamous Ankle Sprain
Now, we've all heard of an ankle sprain and if you don't have first hand experience, you for sure know or heard of someone who has suffered from this. But what does it mean when someone has sprained their ankle? How does one heal from it?
There are 2 types of ankle sprains: inversion and eversion ankle sprains. Inversion is twisting your foot inwards (where the sole of your foot is facing in) and an eversion sprain is twisting your foot outwards (where the sole of your foot is facing out). The first type is the most common.
It usually happens when you "roll" onto the outside of your foot and may have sensed a popping/tearing sensation.They can happen in so many different ways and at different severity's, as outlined below.
There are 2 types of ankle sprains: inversion and eversion ankle sprains. Inversion is twisting your foot inwards (where the sole of your foot is facing in) and an eversion sprain is twisting your foot outwards (where the sole of your foot is facing out). The first type is the most common.
It usually happens when you "roll" onto the outside of your foot and may have sensed a popping/tearing sensation.They can happen in so many different ways and at different severity's, as outlined below.
 |
| Grades of Ankle Sprains from Conditions Manual by Dr. M. Carnes and Dr. N. Vizniak |
But now we know what it is, how do we heal from it? Up to 72 hours after injury, just remember PRICE.
- P - Protect the ankle with splints, tape, or loose lace-up support. Don't want to injury yourself even more now, do we?
- R - Rest by reducing any weight bearing activities, but try to return to activity ASAP (don't want to be resting too long).
- I - Ice 20 minutes on with 1 hour intervals to control any inflammation and reduce secondary injury (this is especially important within the first 24 hours).
- C - Compression. This can be done with elastic wrap or tape, or even keeping your shoe on while on the field (if injured in such a manner) to help with any swelling. If there's little room to swell, the swelling can only go so far!
- E - Elevate your leg to allow you to rest up and help control swelling for the first 48 - 72 hours.
After the first 72 hours, you want to wean yourself off crutches and try to get back to pain free activities. Once you've mastered one activity pain free, try to challenge it a little more. BUT make sure you don't overdo it! We don't want to re-injure ourselves now do we?
A great way would be to start with alternating pointing toes and bringing the toes back while sitting. Once that no longer hurts, then try doing it while you're standing (stand on your tippy toes and back down). Once you've jumped that hurdle, let's go for a walk. It's great weather now, so why not go for a walk, barefoot, on the beach? The uneven surfaces of the beach really challenges those muscles and helps your muscles/ligaments heal much better. Besides, exercising and healing while having the sun shining on your face, breathing the fresh air, and hearing the waves crashing on the shore - can you think of a better way to heal yourself?
Continue with these exercises and continue to challenge yourself once you've reached the "pain free activity" stage until you're pretty much back to your normal self! Now you're able to walk properly again and got a sweet tan, perfect.
To learn more about ankle sprains, how to manage them, or learn about other conditions that can afflict our fabulous bodies, click here to order the Conditions Manual.
Tuesday, 14 May 2013
Carpal Tunnel Syndrome
Carpal Tunnel Syndrome (CTS) is an issue afflicting many people every day, often due to overuse and repetitive movement of the wrist (specifically the flexor muscles). Actions such as typing, massaging and rock climbing are activities known to contribute to this problem.
CTS is caused by entrapment of the median nerve between the flexor retinaculum (a ligament that acts as a pulley for the flexor tendons) and the carpal bones (the two structures making the tunnel). Both the median nerve and wrist flexors run between those two structures, so when inflammation occurs, and neither the flexor retinaculum nor the carpal bones are able to expand to help relieve pressure, the median nerve is ultimately compressed.
Patients with CTS will often present with numbness, tingling, weakness and pain extending from the wrist, into the palm of the hand and up into the thumb, pointer, middle and lateral half of the ring finger. If compression is before the tunnel and the palmar branch is affected, patients will experience symptoms in the middle of the palm. They may also present with the ‘flick maneuver’ to relieve pain which is exactly as it sounds, a flicking of the wrist as though they were trying to get some water off of it.
CTS is caused by entrapment of the median nerve between the flexor retinaculum (a ligament that acts as a pulley for the flexor tendons) and the carpal bones (the two structures making the tunnel). Both the median nerve and wrist flexors run between those two structures, so when inflammation occurs, and neither the flexor retinaculum nor the carpal bones are able to expand to help relieve pressure, the median nerve is ultimately compressed.
Patients with CTS will often present with numbness, tingling, weakness and pain extending from the wrist, into the palm of the hand and up into the thumb, pointer, middle and lateral half of the ring finger. If compression is before the tunnel and the palmar branch is affected, patients will experience symptoms in the middle of the palm. They may also present with the ‘flick maneuver’ to relieve pain which is exactly as it sounds, a flicking of the wrist as though they were trying to get some water off of it.
Compression of the median nerve can occur in numerous other places and it is important to rule them out before confirming CTS. Compression can occur at the vertebrae as the nerve exits, between the scalene muscles, under the clavicle and between the heads of the pronator teres muscle.
For more information on Carpal Tunnel Syndrome, the tests to confirm or rule it out, please refer to Professional Health Systems’ Conditions Manual.
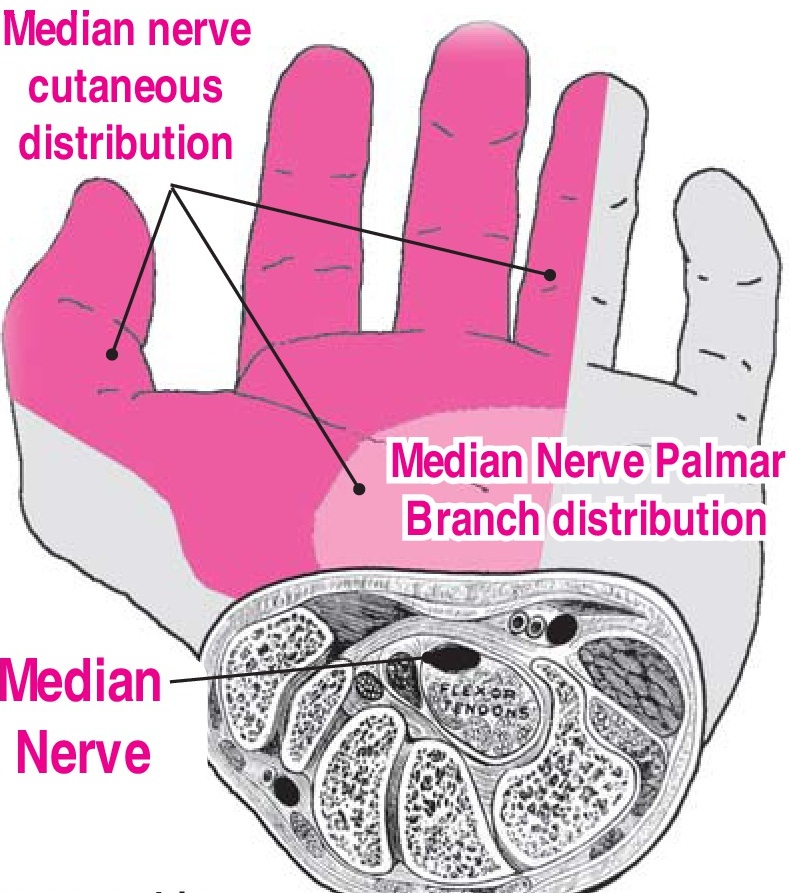
| A section of the wrist displaying the carpal bones, flexor tendons, median nerve (black oval) just above the tendons, and the flexor retinaculum running above those structures. |
Hello! And welcome to Professional Health Systems’ new blog!
We’re excited to have this up and running and also to begin supplying you with new content covering both anatomy, clinical issues and links to any interesting articles we find that we think you may also enjoy.
Supplying the blog will be two students from The Boucher Institute of Naturopathic Medicine- Katherine Chung and Jordan Morton.
To learn more about Professional Health Systems, check out the website! And please contact us with any questions or comments you may have, thanks.